UNDERSTANDING THE PRODUCTIVITY BURDEN OF BREAST CANCER IN AUSTRALIA
Breast cancer in Australia impacts work, income, and wellbeing. Learn about productivity loss, employment disruption, and support for returning to work.
Breast cancer is not only a health crisis – it also disrupts work, income, and identity for thousands of Australians each year. Beyond the physical toll, the productivity burden of breast cancer in Australia includes lost wages, reduced hours, and the economic ripple that effects the wider community.
Recent research by Monash University shows the scale is staggering: working-age Australian women diagnosed with breast cancer collectively lose an average of 1.5 years of full-time work each, costing billions in wages and gross domestic product (GDP). But these numbers only tell part of the story – behind them are the challenges of career disruption, financial hardship, and emotional wellbeing.
This article explores the statistics, human impact, barriers to returning to work, and the resources available to help people rebuild their professional and personal lives after treatment.
Key Statistics on Productivity Loss in Australia
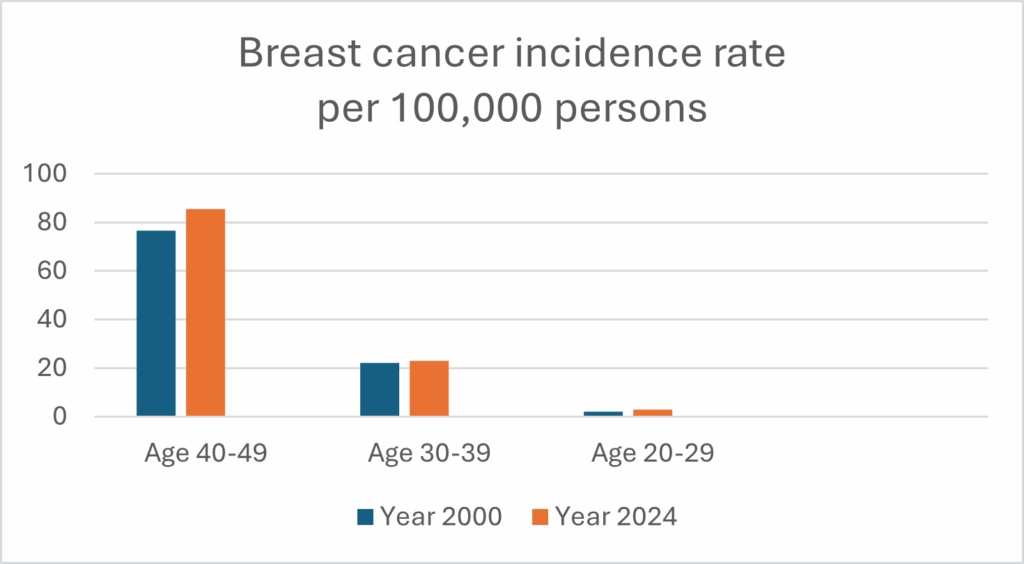
- In 2022, around 10,732 working-age Australians (mostly women) were diagnosed with breast cancer.
- Over the following decade, these individuals are expected to lose 16,403 productivity-adjusted life years (PALYs) – a measure of the economic impact of disease that factors in lost productivity due to time off work, reduced productivity while working and factors that result in premature cessation of work.
- That equates to AU$1.4 billion in lost wages and AU$3.26 billion in GDP losses for Australia.
- On average, each woman loses about 1.5 years of full-time work after diagnosis.
The Monash study also found productivity loss exceeds direct healthcare costs, showing the economic impact of breast cancer extends far beyond hospital bills.
ABC News reports that in the first five years after diagnosis, women may lose around half a year of productivity per year, though this improves with time. Since nearly 40% of cancer diagnoses in Australia occur in people aged 25–64, the ripple effect on the economy is enormous – estimated at AU$1.7 billion annually from employment disruption.
How Breast Cancer Affects People’s Lives and Identity
With the increasing cost of living, a reduction in income or pause in earnings places significant stress on patients, but there are also other factors to consider. For many, work is more than just a paycheck – it’s tied to identity, routine, and purpose. Losing the ability to work, or needing to reduce hours, can affect confidence and increase anxiety about financial stability. This shows the productivity burden of breast cancer is not only economic but deeply personal.
Some common impacts include:
- Financial strain & Financial Toxicity: lost salary, breast cancer out-of-pocket expenses, fewer superannuation contributions, and in some cases debt or bankruptcy.
- Career disruption: missed opportunities for promotions, forced early retirement, or difficulty re-entering the workforce.
- Psychological distress: the emotional weight of job loss or reduced work can contribute to stress, mood disturbance, and reduced quality of life after breast cancer.
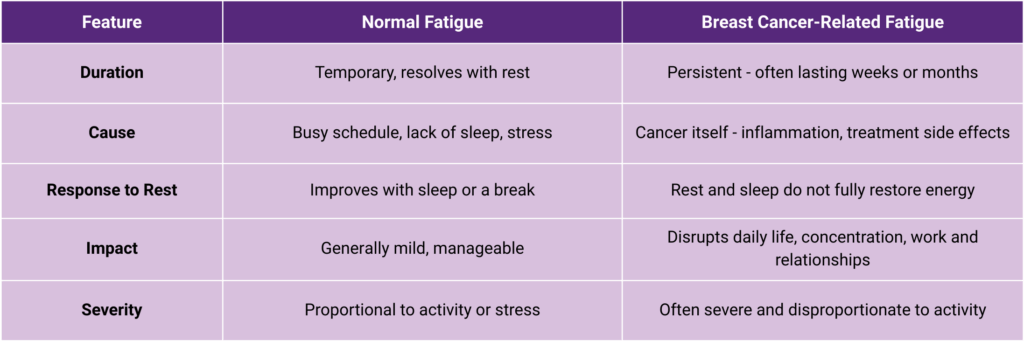
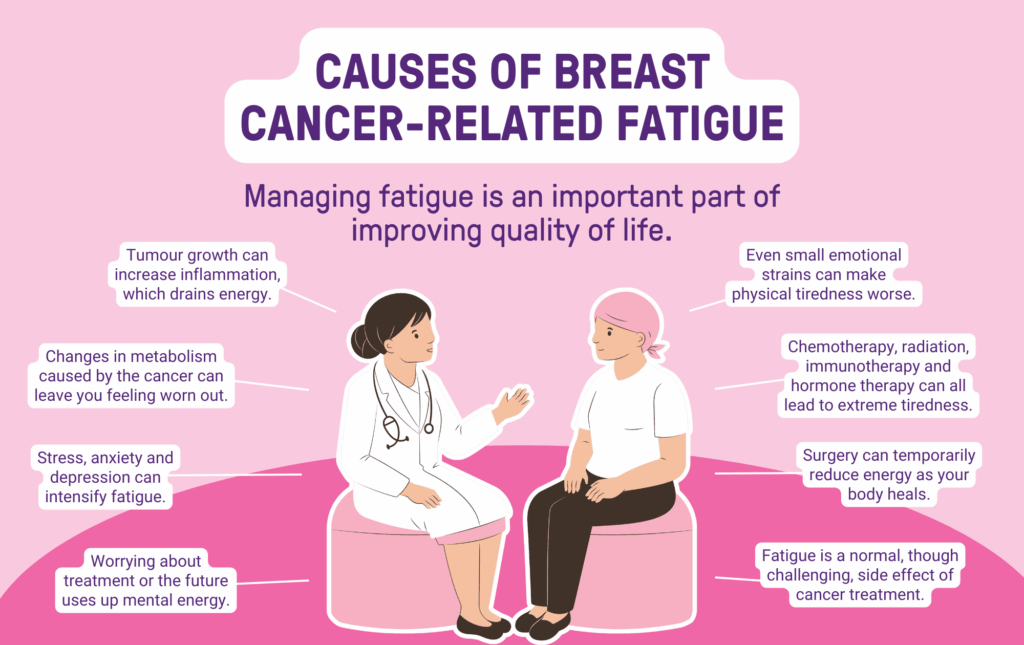
- Long-term side effects: breast cancer and treatment may cause side effects to patients such as fatigue, brain fog, pain, or lymphoedema that can limit work capacity.
Why Returning to Work After Breast Cancer Can Be Challenging
Re-entering the workforce after treatment is rarely straightforward. Barriers include:
- Physical challenges: ongoing treatment side effects such as fatigue, pain, and brain fog.
- Medical demands: follow-up appointments, ongoing medication, and rehabilitation schedules.
- Workplace barriers: limited flexibility, lack of understanding from employers, or even discrimination.
- Emotional readiness: coping with the fear of recurrence and balancing health concerns with career goals.
Cancer Australia highlights that these barriers explain why many patients face prolonged employment disruption and reduced work hours, even years after treatment.
Why Supporting People to Return to Work After Breast Cancer Matters
Helping people return to work is not only about restoring income. It provides:
- Economic benefits: reducing lost productivity, wages, contribution to superannuation and GDP impacts.
- Personal benefits: restoring identity, purpose, and quality of life after breast cancer.
- Social benefits: work provides connection, routine, and a sense of contribution.
As the Monash University research emphasises, supporting women back into the workforce reduces the economic burden of cancer in Australia while improving wellbeing.
Breast Cancer Trials is a leader in quality of life research, with a number of past and current clinical trials that aim to improve the lives of breast cancer patients, during and after their treatment. For example:
- The OPTIMA clinical trial: aims to find out if we can identify patients with ER-positive, HER2-negative early breast, who may not need to have chemotherapy and avoid the potential side effects of this treatment.
- The PROSPECTIVE clinical trial: aims to find out if surgery without radiotherapy will still be effective at stopping cancer from coming back. This also reduces the potential side effects and costs of treatment.
Support Services and Resources for Returning to Work After Breast Cancer
A number of organisations provide free resources to help answer your questions about financial and employment factors, financial burden, legal issues, workplace law and helping survivors reintegrate into the workforce:
- Cancer Council: workplace fact sheets, legal advice, and counselling.
- Breast Cancer Network Australia: resources on employment rights, financial counselling, and coping strategies.
- Cancer Institute NSW: help with financial, work and legal issues.
- Employers: many workplaces offer flexible arrangements such as phased return, remote work, or reduced hours.
Frequently Asked Questions
How long do women typically stop working after a breast cancer diagnosis in Australia?
Many take several months off during treatment. Some return part-time within 6–12 months, while others need longer or are unable to return to work. Monash research suggests each women loses around 1.5 years of work on average.
Can I return to work part-time or with flexible arrangements in Australia?
Many employers support phased or flexible returns. Options include reduced hours, remote work, or flexible scheduling. The Cancer Council and BCNA recommend creating a return-to-work plan with your employer.
What legal protections support employees returning to work after cancer in Australia?
Under the Fair Work Act and Disability Discrimination Act, employers must provide reasonable adjustments. You cannot be discriminated against for having breast cancer or ongoing treatment.
What support services are available to help women get back to work after breast cancer treatment?
The Cancer Council provides workplace fact sheets and legal advice. BCNA offers guidance on employment and financial counselling. Government and superannuation programs may also help.
Join Our Free Q&A Webinars
Don’t miss an opportunity to stay informed about the latest in breast cancer research and care. Join our FREE Q&A webinars, where we cover important topics including whether more young women are being diagnosed with breast cancer
Stay Connected with Breast Cancer Trials
Don’t miss an opportunity to stay informed about the latest in breast cancer research and care. Sign up to our researcher’s newsletter via the form below to stay up to date.