Breast Cancer Fatigue vs Normal Fatigue: What You Need to Know
Learn how breast cancer fatigue differs from normal tiredness. Trusted information to help patients and caregivers understand and manage fatigue.
Fatigue is one of the most common and challenging symptoms experienced by people with breast cancer, yet it is often underestimated. Unlike normal tiredness, breast cancer-related fatigue can be overwhelming and persistent, affecting every part of a person’s daily life.
This article explores the differences between breast cancer-related fatigue vs normal fatigue, why these differences matter, and how patients and caregivers can better understand and manage this symptom.
What is Breast Cancer-Related Fatigue?
Breast cancer-related fatigue is a persistent, distressing sense of physical, emotional and/or mental exhaustion that is disproportionate to recent activity and is not relieved by rest or sleep.
This is one of the most common and challenging aspects of breast cancer and it often affects daily life more than people expect. Individuals experiencing this type of fatigue may notice a loss of energy that impacts their ability to concentrate, work, socialise, exercise, or even manage basic household tasks.
Unlike normal tiredness, which is usually resolved with rest, breast cancer fatigue can last for weeks or months with no real relief.
Causes of breast cancer-related fatigue include:
- Biological factors: cancer burden, inflammation and changes in metabolism caused by the breast cancer itself.
- Psychological factors: stress, anxiety, and depression can significantly contribute to exhaustion.
- Treatment-related factors: chemotherapy and immunotherapy, radiation therapy, surgery, and hormone therapy are all known to cause fatigue.
Recognising and managing fatigue is an important part of improving quality of life for people with breast cancer. Breast Cancer Trials is dedicated to research that not only finds better treatments and prevention strategies but also improves the quality of life of patients during and after treatment.
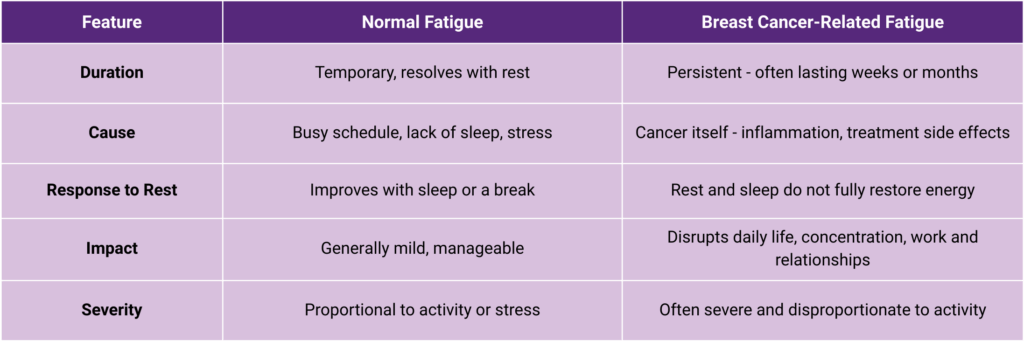
Breast Cancer-Related Fatigue vs Normal Fatigue
Understanding the distinction between normal fatigue vs breast cancer fatigue is necessary for both patients and caregivers.
Scenario: A person with normal tiredness may feel refreshed after a weekend off. Someone with breast cancer fatigue may wake up exhausted despite sleeping for 10 hours.
Patients often share similar experiences on forums such as reddit, which helps validate these feelings for others living through it. One patient described their experience:
- “I am exhausted. This is my 3rd day off, and I still feel utterly shattered. I know not sleeping well doesn’t help, but my body feels devoid of energy.” – shared in an online support forum.
BCNA have an online network where patients share their experiences with breast cancer fatigue.
- “I remember the fatigue from radiation was overwhelming at the end. I remember sitting at the traffic lights thinking l wonder if l just put my head down on the wheel would anyone notice. Worst ever tiredness. Sleep sleep and more sleep.” – Adean.
Hearing real-life experiences like this reassures people that they are not alone – and that what they are experiencing is a recognised symptom of breast cancer, not simply a sign of “not trying hard enough.” This distinction is important for self-compassion, for seeking appropriate medical advice, and for ensuring fatigue is addressed as part of holistic breast cancer care.
Does Breast Cancer Make You Tired?
Breast cancer can cause significant tiredness, even before treatment begins. This is often surprising for patients who expect fatigue to be linked only to treatments such as chemotherapy or radiation therapy, but the cancer itself can cause profound tiredness.
Why does breast cancer cause fatigue?
Fatigue in breast cancer is often multi-factorial, meaning there are several overlapping causes:
Biological factors
- Cancer cells consume a significant amount of the body’s energy as they grow and divide.
- The presence of cancer triggers the release of chemicals called cytokines, which are part of the immune system’s inflammatory response. These chemicals can disrupt how your body produces and uses energy, leading to fatigue.
Emotional and psychological stress
- A breast cancer diagnosis can lead to heightened anxiety, stress and even depression, all of which can drain energy levels.
- Sleep is often disrupted by worry, contributing further to tiredness.
Physical changes
- Pain or discomfort caused by the tumour itself can make it harder to rest properly.
- Appetite loss, nausea or changes in eating patterns can reduce calorie intake, leaving the body with less fuel for daily activities.
What Stage of Breast Cancer Causes Fatigue?
Breast cancer fatigue can occur at any stage of breast cancer, from early diagnosis to advanced disease. It is not limited to later stages or to periods during treatment.
For many with early breast ancer, fatigue may occur even before treatment begins. This can be caused by the physical effects of the breast cancer on the body, such as:
- Inflammation and changes in metabolism
- The emotional impact of receiving a diagnosis.
- Diagnosis shock – the stress, anxiety and disrupted sleep that often follow the news can significantly drain energy and contribute to early fatigue.
With metastatic breast cancer, fatigue may become more severe due to a higher cancer burden, more intensive treatment, or complications from the disease like pain. However, it’s important to note that even when the cancer is small or localised, the body’s immune and stress responses can still trigger significant tiredness.
When considering which stage of breast cancer causes fatigue, it is less about pinpointing one phase of illness and more about understanding that fatigue is possible at any point. This knowledge helps patients and caregivers take symptoms seriously, seek support early, and manage fatigue as part of comprehensive breast cancer care.
Breast Cancer Fatigue Before Treatment Begins
Fatigue can occur at any stage of breast cancer – and for some people, it appears well before treatment begins. This early fatigue can be driven by a mix of physical changes caused by the cancer itself and the emotional impact of receiving a diagnosis.
Fatigue before breast cancer diagnosis – physiological changes
Before treatment starts, the body may respond to an emerging tumour with inflammatory changes that can disrupt metabolism, leading to loss of energy and significant tiredness. Immune system activation and hormonal disruption, such as changes in cortisol, can also cause breast cancer fatigue symptoms even before treatment begins.
In the CANcer TOxicity (CANTO) cohort study, 24.3% of women with stage I to III breast cancer reported severe fatigue at diagnosis – before any treatment had begun. This shows that early-stage breast cancer and fatigue are linked, and that early-stage breast cancer can cause fatigue.
Breast cancer fatigue before treatment – emotional impact
The period immediately after a breast cancer diagnosis can also be exhausting on an emotional level. Diagnosis shock – with its stress, anxiety, disrupted sleep, and emotional upheaval can cause a persistent “mental fog” that makes daily life feel overwhelming. For some, this emotional strain combines with existing physical tiredness, leading to breast cancer fatigue before treatment has begun.
Recognising fatigue before treatment validates patients’ experiences and ensures it is addressed early. By acknowledging that both physical and emotional factors can drive fatigue before a single treatment session has begun, patients can be offered supportive care strategies sooner, improving quality of life from the very start of their breast cancer journey.
Fatigue During and After Breast Cancer Treatment
Radiation Therapy and Fatigue
Fatigue from radiation therapy for breast cancer usually develops gradually rather than appearing suddenly. For most patients, it starts as mild fatigue in the early weeks, then peaks toward the end or even after the treatment course is completed. This is due to the body’s need to repair the healthy tissue that is also affected by radiation, alongside the effect of radiation on the cancer cells.
How long fatigue lasts after radiation for breast cancer varies from person to person. Many people notice improvement within two to four weeks after finishing treatment, but for others, fatigue can persist for several months as the body continues to recover.
Practical ways to manage radiation-related fatigue include:
- Staying well-hydrated to support overall health and energy.
- Engaging in gentle physical activity, such as walking or stretching, which research shows can help restore energy levels.
- Prioritising rest and scheduling tasks for times of day when energy is highest.
Breast Cancer Trials EXPERT trial is exploring whether the Prosigna genomic test of breast cancer tissue can identify women who can safely avoid radiation therapy after breast cancer surgery, potentially avoiding the fatigue it can cause. The PROSPECTIVE trial is another radiotherapy omission trial, examining whether MRI can detect patients who can be successfully treated with surgery without radiotherapy, reducing side effects like fatigue and lowering the overall treatment burden.
Surgery, Chemotherapy, and Hormone Therapy Fatigue
Different breast cancer treatments can cause fatigue in different ways. The type, timing, and intensity of fatigue will depend on the treatment and the individual.
Surgery
Post-surgery fatigue is common due to the body’s healing process, the lingering effects of anaesthesia, and pain medications. Recovery may take several weeks, and for some people, emotional stress can make tiredness more noticeable.
Chemotherapy
Chemotherapy often leads to intense, prolonged fatigue because it impacts healthy cells as well as cancer cells. Immune suppression, anaemia, and the body’s efforts to clear treatment toxins all contribute to low energy.
The OPTIMA trial is testing whether the Prosigna genomic test of breast cancer tissue can help identify individuals who can safely avoid chemotherapy and its potential side effects, including severe fatigue, when the treatment is unlikely to provide additional benefit.
Hormone Therapy
Hormone therapy, typically taken for years after initial treatment, can lead to ongoing low-grade fatigue due to hormone changes, particularly reduced oestrogen. These changes can affect sleep quality, mood, and overall energy balance.
Is Fatigue a Sign of Breast Cancer Recurrence?
While fatigue is a common symptom of breast cancer, fatigue alone is rarely a sign of breast cancer recurrence. However, new or worsening fatigue should be discussed with your medical practitioner.
Other symptoms to watch for include:
- New pain or lumps.
- Unexplained weight loss.
- Persistent nausea or other changes in health.
How to Manage Breast Cancer-Related Fatigue
Feeling a persistent lack of energy and motivation is one of the most frustrating aspects of breast cancer-related fatigue. For many people, it’s not just physical tiredness – it’s also the lack of motivation or energy to take part in the activities they once enjoyed. Even simple daily tasks can feel overwhelming, leaving you feeling constantly tired and unable to recharge.
Managing breast cancer-related fatigue symptoms requires a versatile approach:
- Gentle exercise (like walking or yoga) can help maintain energy.
- Prioritise quality sleep and rest.
- Maintain a balanced diet – read dietitian Dr Cindy Tan’s advice.
- Keep a fatigue diary to track patterns.
- Access emotional support and counselling.
If fatigue is persistent, worsening, or affecting the ability to carry out daily activities, it’s time to seek professional support. This is especially important if fatigue is accompanied by other symptoms like breathlessness, dizziness, or unexplained pain.
Through Breast Cancer Trials’ research program we’re exploring ways to better understand and manage side effects like fatigue, and shape future treatments.
When to Seek Help for Breast Cancer Fatigue
Fatigue is more than just tiredness. Seek medical advice if fatigue:
- Interferes with daily tasks like bathing, eating or walking.
- Is worsening over time.
- Impacts your safety (e.g. falling asleep at work or while driving).
Managing fatigue is part of holistic breast cancer care. Your doctor can help rule out other causes like anaemia or thyroid issues.
Frequently Asked Questions
Does breast cancer make you tired before treatment?
Yes, many patients report fatigue even before treatment begins. This early tiredness can be caused by the body’s immune response to the tumour, inflammation, and the stress of the diagnosis process. The emotional impact – including shock, anxiety, and disrupted sleep – can also contribute.
How long does fatigue last after radiation treatment for breast cancer?
Fatigue from radiation therapy often builds gradually during the treatment course and peaks toward the end. Most people experience tiredness for several weeks after treatment finishes, though in some cases it can persist for a few months. The length and severity of fatigue depend on factors such as treatment intensity, duration and overall health.
Can early stage breast cancer cause fatigue?
Yes, even early-stage breast cancer can cause fatigue. The cancer itself may release substances that affect metabolism and energy production, while emotional stress, anxiety, and sleep disruption around the time of diagnosis can add to the problem.
Is fatigue after surgery normal?
Yes – fatigue is very common after breast cancer surgery. It can be caused by the body’s healing process, the lingering effects of anaesthesia, pain medications, and emotional stress. For most patients, energy levels gradually improve over time, but some may continue to feel tired for weeks or even months post-surgery.
How can I tell if my fatigue is normal or breast cancer-related?
Breast cancer-related fatigue is typically persistent and not relieved by rest or sleep. It may feel overwhelming and affect concentration, emotions, and physical ability. If you are tired all day despite getting enough sleep, or if fatigue is interfering with your daily life, it could be cancer-related.
Sources:
https://forum.breastcancernow.org/t/normal-fatigue/132672?
https://onlinenetwork.bcna.org.au/discussions/side-effects/fatigue/178218
clinical-breast-cancer.com+4sciencedirect.com+4ascopost.com+4cheneyclinic.com
https://ascopost.com/news/february-2022/predictive-model-for-severe-fatigue-after-breast-cancer-diagnosis/
Join Our Free Q&A Webinars
Don’t miss an opportunity to stay informed about the latest in breast cancer research and care. Join our FREE Q&A webinars, where we cover important topics like managing treatment side effects and supportive care.
On September 24, we will be discussing the side efects of treatment.
Stay Connected with Breast Cancer Trials
Don’t miss an opportunity to stay informed about the latest in breast cancer research and care. Sign up to our researcher’s newsletter via the form below to stay up to date.